
What GLP-1 drug price is cost neutral to Medicare?
Seemingly around $140/month

As GLP-1s are studied more, their benefit profile is expanding rapidly. Acknowledging that many questions remain, a recent journal article titled The expanding benefits of GLP-1 medicines puts it like this:
GLP-1 medicines, initially developed for blood glucose and weight control, improve outcomes in people with cardiovascular, kidney, liver, arthritis, and sleep apnea disorders, actions mediated in part through anti-inflammatory and metabolic pathways, with some benefits partly independent of the degree of weight loss achieved.
Many millions of Americans would benefit from taking these drugs, but limited insurance coverage and high out-of-pocket costs limit their use. However, if the price was low enough to match their cost savings, then wider coverage could be justified.
What price would that need to be?
How can a drug be cost neutral (pay for itself)?
If a drug reduces future care expenditures by more than it costs, then it pays for itself (is cost neutral). Modeling this out can get complicated, especially for drugs whose benefits accrue over many years. That’s because you need to at least consider how those cost savings unfold as well as people who stop taking the drug (adherence rate).
What about GLP-1s?
The Congressional Budget Office (CBO) looked into this question in detail in 2024, using these approximate assumptions:
9-year time horizon (2026-2034)
35% adherence (continuation) in first year, ramping up to 50% by year 9
80% yearly continuation rate after first year of continuous use
Available to Medicare patients who are classified as obese or overweight with at least one weight-related comorbidity
$5,600/year cost (implying about ~$625/month cost if you assume a 75% reimbursement)
Savings from reduced care of $50/year in 2026, reaching $650/year in 2034
CBO concludes in their report that these assumptions lead to expanding GLP-1 coverage to be very costly to the Federal government.
Doesn’t Medicare prescribe GLP-1s now?
Yes, but not for obesity writ large, which about doubles the qualified population. From the CBO report:
In 2026, in CBO’s estimation, 29 million beneficiaries would qualify for coverage under the illustrative policy. About half of that group, or 16 million people, would have access to those medications under current law for indications such as diabetes, cardiovascular coverage, and other indications approved by the FDA in the interim.
Still, CBO only expects a small percentage of eligible patients to use the drugs, due to activation and adherence. In the final year of their model (2034) they predict “about 1.6 million (or 14 percent) of the newly eligible beneficiaries would use an AOM [anti-obesity medication].”
What break-even price does the CBO report imply?
CBO doesn’t calculate a break-even price. They just say they expect $50 in average savings in year 1, rising to $650 in year 9, implying a 9% offset rate overall. If we assume a progression of increasing yearly savings to match these assumptions, you get a cumulative savings of about $4,000, or about $445 per year. If you assume on average the government picks up 75% of the bill, that implies a break-even drug price of about $50/month.
What has changed since 2024 that would modify this CBO estimate?
Time Horizon. The CBO time horizon of 9 years is too low. They acknowledge that “from 2035 to 2044…the savings from improved health would be larger than they would be from 2026 to 2034”. So, let’s add 10 years (for a total of 19), and stipulate the last ten years average $800 in savings, rising from the year 9 savings of $650. That implies an increased average savings per year of about 1.4x.
Emerging Benefits. The CBO only accounted for weight-loss benefits, using comparisons to Bariatric surgery and other weight-loss evidence, noting that “CBO is not aware of any direct evidence showing that treatment of obesity with GLP-1-based products reduces spending on other medical services.” However, the other emerging benefits reduce conditions that are very costly to Medicare like kidney, heart, and sleep apnea complications (e.g., dialysis, heart surgery, CPAP, etc.). I think we can speculatively call this a 2x multiplier.
So, then what break-even price does that imply today?
$50/month (CBO original estimate) x 1.4 (for increased time horizon) x 2 (for increased benefits) =~ $140/month.
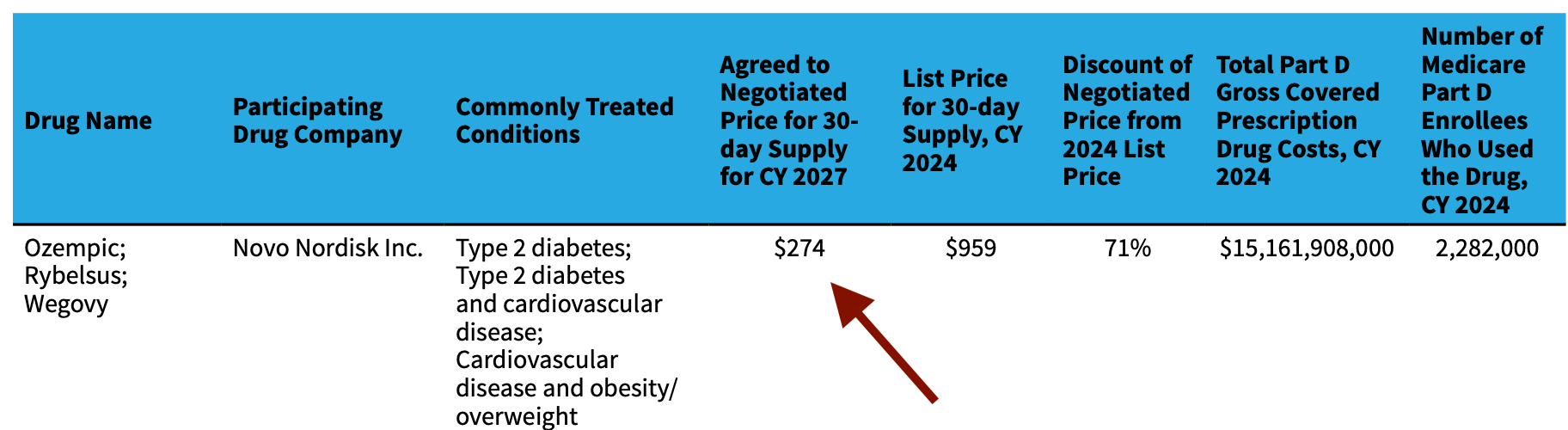
That is, at $140/month, we would expect the Medicare costs to roughly equal the cost savings, and net out to 0 (be cost neutral). That’s still well below the recently negotiated prices starting in 2027 (for example, Ozempic at $274).
Why are you thinking about this again?
I’m seeing the expanding benefit profile and thinking we have to find a way to get these benefits to more people, as a way to generally increase our average standard of living (in this case by greatly increasing health-span/quality of life).
The best way I can see to get the benefits to the most people is if it were government subsidized/provided. But obviously health care costs are a major barrier to that method, and so framing expanding benefits as cost neutral seems most politically viable.
What if the price were $100/month?
At $100/month, then it would be a no-brainer (assuming the above math is correct) to make available to qualified Medicare patients (say, using at least the CBO obesity criteria) since it would then be clearly making the government money.
Additionally, at that price, I think you could start expanding it well beyond Medicare in waves, monitoring outcomes and cost savings. For example, you could start with programs where the government similarly runs both the cost and benefits like Medicare, such as for the military and other federal workers. Then you could expand to Medicaid / disability (with cross-state subsidies). Ultimately there could be justification to subsidize a subset of the public at large, for example people aged 55+ who will be on Medicare within the next ten years, such that the savings will be realized by the federal government and the whole program could still be cost neutral.
OK great, but how to you get GLP-1s at $100/month?
This may be a half-baked idea, but one approach is to offer up the market a yearly contract for expanded Medicare, and whoever shows up first gets it (to be renegotiated yearly).
I don’t think this is that crazy because the manufacturing cost is estimated to be a small fraction of the list price, and the UK previously had negotiated pricing in this ballpark. The volumes would be huge, and as more companies enter the market, I imagine eventually one of them would take the offer.
Beautiful analysis. Did the report calculate the increase in costs from longevity? (You know the actuaries do!) For example, if people taking GLP-1 drugs get fewer heart attacks and strokes, will more of them be getting joint replacements?
© Substack Inc